ASOURCE®TIMES
淡海医療センター(滋賀県草津市)では、2019年に多くの医療データを包括的に収集・分析するシステム、コマンドセンターを日本で初めて導入し、看護師の業務効率や病床稼働率の向上などに成果を上げています。統括看護部長の伊波早苗氏にコマンドセンターの導入の経緯、電子カルテデータの活用法や導入後の業務の変化について伺います。
以前から、電子カルテ上の情報をうまく利用することで看護の労務効率を向上できるはずと常々感じていました。例えば、入退院数から病棟に配置すべき看護師数を割り出すために毎日電卓を使って計算していましたが、これが自動化できればほかの業務に時間を使える、こういった希望を当院の経営管理担当部長に相談していました。
その経営管理担当部長が医療機器メーカーの日本法人の米国研修でジョンズ・ホプキンズ病院のコマンドセンターを見学し、日頃私が話している課題が解決できるとして当院での導入を進言してくれました。経営陣もこれを了承し、2019年に導入が決まりました。
コマンドセンターとは、電子カルテなどの病院内の情報を統合し、包括的に解析して、病床の稼働、ケアやタスク、人員配置など必要な情報をリアルタイムで表示するシステムです。
ジョンズ・ホプキンズ病院のコマンドセンターは、主に救急車の運行やスタッフ配置を“見える化”する地域医療向けのシステムでした。それを日本の病院医療向けに仕様変更するために、医療者ではない医療機器メーカーの担当者に理解してもらいつつ、仕事のプロセスを見直しながら、半年間かけてオリジナルのシステムを構築しました。システムが動き始めたときは、電子カルテのデータ格納や取り出しがうまくいかず、さらに半年ほど調整に時間を要しました。

コマンドセンターは、毎朝、病棟看護師長が病床コントロールのミーティングをする会議室に設置。
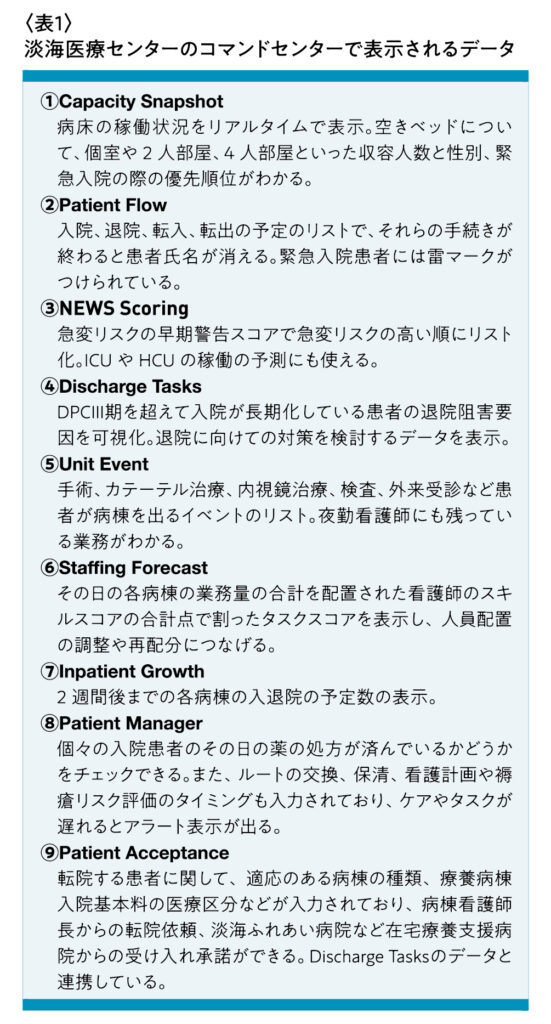
コマンドセンターはデータの統合分析サーバと複数のタイル(Tile)と呼ばれるアプリケーションで構成されており、このタイルを通じて病床管理・入退院支援に必要となる院内データを分析・可視化し、ケア需要の予測、施設間の移動、ケアの進行、退院計画など、刻一刻と変化する患者さんの状況をタイムリーに捕捉することで、医療従事者の高品質かつスピーディーなケアの実現をめざしています。タイルの数や種類は、施設の規模やニーズに即して変更できるモジュール形式になっており、現在、当院では10画面のモニターを設置し、表1の①〜⑨を表示しています。①のCapacity Snapshotは2画面を使っています。
病棟看護師の働き方は、病床の稼働状況、患者ごとあるいは病棟全体のケアやタスク、看護師の数やスキルが可視化されることで、大きく変わりました。
例えば、⑥Staffing Forecastでは、病棟ごとの業務と看護師の配置数が一体化されたデータとして見ることができます。この画面では、手術、カテーテル検査などの数、ドレーンや人工肛門を装着している患者数、転倒・転落リスク、認知症の有無、新規入院患者のオーダーなどがリスト化、点数化されています。さらに、病棟看護師の経験年数、役職、能力などの評価スコアを組み合わせ、病棟のタスクスコアが計算されて15分ごとに自動更新されます。
現時点では、このタスクスコアが25点を超えるとその病棟への応援が必要な状況と判断しています。これによって、タスクスコアが低い病棟からタスクスコアの高いより忙しい病棟に看護師が自発的に応援に行くようになったことが、コマンドセンター導入の最も大きな成果の一つだと考えています。また、担当外の病棟に行くことで、そこで新しく学んだよりよい方法を担当病棟でも取り入れたり、物品の置き場を共通にしたりといった動きもありました。
こうして業務を可視化し、働き方を変えたことで、一般急性期病棟の1ヵ月あたりの総残業時間はコマンドセンターの稼働前の2020年と比較して2021年は、コロナ禍の最中にあっても44%(月当たり約1035時間)削減しました。また、病棟ごとの超過勤務時間の格差についても改善が見られました。標準偏差で見ると、以前は240時間あったばらつきが、現在では78時間まで縮小しています。特に、最も超過勤務時間が多かった病棟では、764時間から331時間へと大幅に減少し、病棟による業務負担の調整が進んでいます。
③のNEWS Scoringは個々の患者を早期警告スコアで評価し、急変リスクが高い順にリスト化したもので、各病棟でも常時掲示しています。血圧などのバイタル測定の結果は測定機器に各看護師が持つスマートフォンをかざすことで電子カルテに自動入力されそれが早期警告スコアに反映されます。同じ画面をICUやHCUの医師がチェックし助言してくれたり、医師が自分の担当外の患者さんの様子も目配りして処置してくれたりすることもあります。このデータを利用することで、患者の状態悪化が激減しました。
病床の稼働状況がリアルタイムでわかり、入退院や転出、転入に必要なケアやタスクもリスト化されているため、導入以前には90%台前半だった病床稼働率も、現在では100%超になっています。
コマンドセンターの導入には、病院経営や医療安全の向上、看護師の残業減少、入退院や転入、転出をスムーズにするというさまざまなメリットがありました。
また、看護師たちが管理職に自分たちがどれだけ忙しいかを理解してもらえるようになったと感じ、自分の病棟も他の病棟も適正な働き方ができるようにと考えられるようになったことも成果の一つでした。
今後は、コマンドセンターに集まるデータを生かしつつ、看護師の情報収集を簡便にするシステムの導入なども検討する予定です。