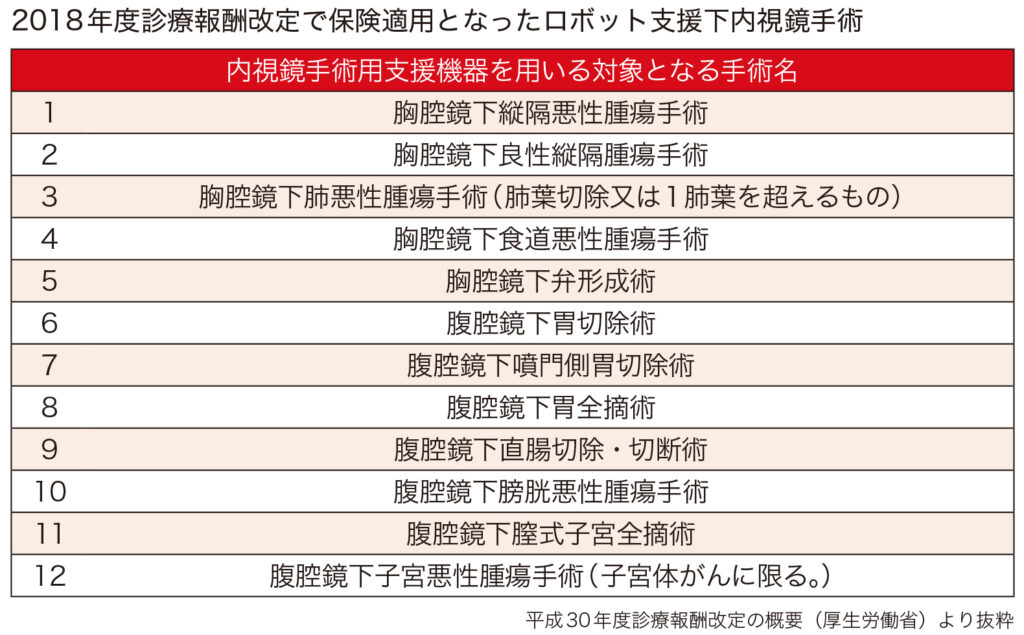
This year's revision of medical care fees has made 12 surgeries using surgical support robots "Da Vinci" newly covered by insurance. This brings the total to 14, including the two surgeries that were previously covered by insurance. In addition to urology, the medical departments involved have expanded to five: gastroenterological surgery, gynecology, respiratory surgery, and cardiovascular surgery. With this latest insurance coverage, medical fees are the same as for regular laparoscopic surgery, and there is no surcharge for using the robot. We looked into the future development of robotic surgery with the expansion of insurance coverage.

Insurance was first applied to total prostate cancer resection in 2012, and expanded to partial resection of kidney cancer in 2016. This time, gastric cancer, lung cancer, esophageal cancer, rectal cancer, bladder cancer, uterine body cancer, mediastinal tumor, valvuloplasty such as mitral valve insufficiency, total hysterectomy, etc. were targeted ( table). Of the 12 cases covered by insurance this time, one (gastrectomy) was already performed in "advanced medical care B", but the other 11 cases were covered by insurance without going through advanced medical care. At present, the scientific basis for superiority of da Vinci surgery compared to existing techniques has not been established, but it is considered to be as effective and safe as possible, and the operability of the endoscope and patients It was evaluated from the viewpoint of expanding the options of the operation, and it is thought that it led to the expansion of the application this time. Another factor is that each academic society has strongly requested insurance coverage for da Vinci surgery.
Currently, da Vinci surgery is most often performed in the urology area. Total resection of prostate cancer and partial resection of kidney cancer, which are already covered by insurance, are evaluated to be more useful than open surgery and ordinary laparoscope, and medical fees are added. More than half of total prostatectomy is done by da Vinci surgery. After removing the prostate, the bladder and urethra are anastomosed, but compared to the rod-shaped forceps used in normal laparoscopic surgery, the tip of the forceps bends freely, enabling fine forceps operation even in deep pelvis. , Because the anastomosis can be surely performed. The number of operations for partial resection of renal cancer is increasing, and it is being confirmed that it is superior to ordinary laparoscopic surgery in terms of renal function preservation and cancer radical resection rate. Bladder cancer, which is newly covered by insurance this time, seems to be spreading quickly because there are many doctors who are proficient in da Vinci surgery in this area. Especially when the bladder is removed, urinary diversion is required, and it is thought that the technique unique to da Vinci surgery can be demonstrated.
In the field of gastrointestinal surgery, "gastrectomy", which was the advanced medical treatment B, is expected to increase steadily. More precise surgery is possible for "rectal surgery", and it is expected that the function-preserving rate of nerves related to postoperative defecation, urination, and sexual function will be higher than that of normal laparoscopic surgery.
In the field of cardiac surgery, da Vinci surgery is difficult to perform, and the facility standards set by the Ministry of Health, Labor and Welfare require a record of 100 open heart surgery and 20 small incision heart surgery annually. Mitral regurgitation was covered by insurance, but Atsushi Amano, director of Juntendo University Hospital, said, "In general endoscopic surgery using a laparoscope or thoracoscope, suturing and ligation are performed. Precise sewing and tying with threads in a space that is difficult and has a narrow field of view is quite a hurdle. On the other hand, in Da Vinci surgery, suturing and ligation can be easily performed by a system that supports fine movements. ". Currently, only a few facilities use Da Vinci for heart surgery, and it will take a considerable amount of time to spread. In the field of gynecology, there are many doctors who are interested, but there are few facilities, and it seems that it will take time to spread. In the field of respiratory surgery, thoracoscopic surgery is performed in about 90% of all cases. The advantages of performing da Vinci surgery are not clear, and it is expected that it will gradually spread while considering safety.

According to the total of the Japan Robotic Surgery Society, the breakdown of the number of da Vinci surgery at the end of 2015 is 12,404 for urinary organs, 544 for digestive organs, 170 for gynecology, and 110 for thoracic surgery. In terms of the number of cases in medical institutions in recent years, Tokyo Women's Medical University Hospital, Juntendo University Hospital, Juntendo University Hospital, Fujita Health University Hospital, Tokyo Medical University Hospital, etc. occupy the top positions. It is expected that the number of experienced facilities will gradually increase with the expansion of this application. It is said that the number of Da Vinci in Japan is close to 300. On the other hand, in the United States, as of 2014, there were far more cases of urinary system 91,000, digestive system 107,000, and gynecology 235,000. Da Vinci surgery is functionally suitable for deep and narrow pelvic surgery, and has the highest number of gynecological cases in the United States. Indications range from benign and malignant tumors, and endometrial cancer is said to have a large number of patients. In Japan, ordinary laparoscopic surgery is widely performed, and there are few facilities that perform da Vinci surgery.
The problem with da Vinci surgery is that the surgeon may accidentally press the organ strongly because the feeling that the instrument touches the organ is not transmitted to the doctor's hand, so great care is required. Also, in the early models, there was interference between the arms (in the latest model, the arms are thinner and the interference between the arms is reduced). Skilled skills of doctors are required to prevent accidents peculiar to robots, and it is urgent to create a system to prepare a training environment for training surgeons. Currently, there are training facilities at the sales company Intuitive Surgical and Fujita Health University Hospital, but it is said that they are filled with reservations until October.
With this insurance coverage, the medical fee is the same as for normal arthroscopic surgery, and there is no additional charge for using a robot. The application greatly reduces the burden and is good news for patients. However, for the hospital side, in addition to the main unit price of 200 to 300 million yen, disposable surgical instruments and maintenance costs (about 25 million yen per year) are not a small burden. If the application increases the number of cases and shows superiority compared to existing technology in clinical trials, it may lead to additional points in medical fees. Mr. Amano said, "Including maintenance and depreciation, da Vinci surgery will not be profitable at present. One measure is to increase the number of patients from overseas who can claim free medical care." There is.
Several companies both in Japan and overseas are developing surgical support robots with almost the same functions as the Da Vinci, and they are expected to be released for sale in a few years at a price of around 100 million yen. It seems that the emergence of low-cost, high-performance surgical support robots is not far off.
The challenge of home medical care that "supports daily life" - A "triple win" for patients, medical institutions, and the government will ensure the future of an aging society...

Supporting the career advancement of female doctors Introduce career counseling to increase the number of female doctors aiming to become specialists...

The new value of medical care is to improve the happiness of patients and medical professionals by providing medical services that emphasize "emotional value"

The introduction of Japan's first command center has changed the way nurses work and increased hospital bed occupancy rates

Informed consent in the medical field as seen through court cases (Part 2)