ASOURCE®TIMES

東京医科歯科大学 特任教授
東京医科歯科大学 M&Dデータ科学センター長
宮野 悟
1977年九州大学理学部数学科卒業。理学博士。1993年九大理学部教授、1996年東京大学医科学研究所ヒトゲノム解析センター教授、2014年ヒトゲノム解析センター長、2015年神奈川県立がんセンター総長などを歴任。2020年から東京医科歯科大学に新設されたM&Dデータ科学センター長。国際計算生物学会(ISCB)ISCB Fellow。2016年度上原賞(「先端ゲノミクスによる癌の分子基盤の解明」)、2019年度ヘルシーソサエティ賞(パイオニア部門)受賞、2023年度大川賞(「スーパーコンピュータを活用した全ゲノム解析、がんゲノム研究の先進的な研究」)受賞。
2023年6月に「良質かつ適切なゲノム医療を国民が安心して受けられるようにするための施策の総合的かつ計画的な推進に関する法律」(通称ゲノム医療推進法)が施行され、個人のゲノム情報を使って治療を個別化するゲノム医療に注目が集まっています。長年、ゲノム情報をはじめとする医療データの収集や利活用に関する研究をリードしている東京医科歯科大学の宮野悟特任教授にゲノム医療の今と未来について伺います。
「ゲノム医療推進法」では、ゲノム医療を「個人の細胞の核酸を構成する塩基の配列の特性又は当該核酸の機能の発揮の特性に応じて当該個人に対して行う医療をいう」と定めています。ゲノム医療が最も進んでいる領域は、がんです。がんは遺伝子が傷ついて起こる病気であることが1970年代に明らかになり、がんの種類や進行度によって異常をきたす遺伝子の種類や数、異常の形式(塩基の入れ替わりやコピー数の異常、染色体の構造異常など)はさまざまで、同じ臓器のがんでも患者さん個人によって異なることがわかってきました。このような遺伝子異常をターゲットとする分子標的薬が開発され、患者さんの遺伝子異常を調べることがスタンダードになってきました。
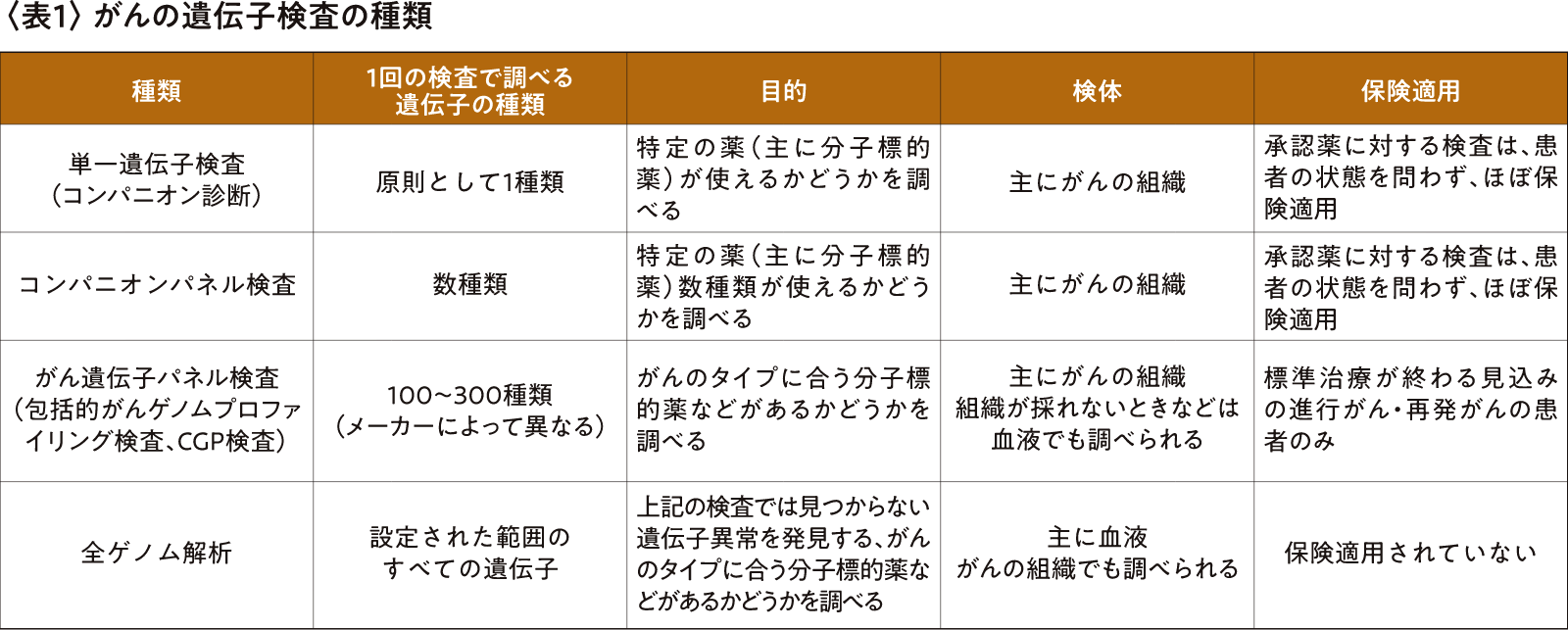
現在行われている、がんの遺伝子に関する検査は表1の通りです。
2019年にがん遺伝子パネル検査が保険適用されがんゲノム医療中核拠点病院などのがんゲノム医療の体制が整備されたことによって、遺伝子検査の取り扱いが容易になり、エキスパートパネルに入る専門家、遺伝腫瘍医や遺伝カウンセラーなどの人材育成が進みました。
一方で、現状では、患者さんががん遺伝子パネル検査を受けられる病院に行き、説明やカウンセリング、検査を受け、結果を受け取って治療方針を決めるまでには最低でも1か月かかります。保険適用されているのは標準治療が終わる見込みの再発がんか進行がんの患者さんのみで、受けられる回数も一度だけという制限があります。検査を受けて適合する薬が見つかる患者さんは10〜15%程度で、また薬が見つかってもすでに体調が悪化していて治療が受けられない患者さんもいらっしゃいます。
がん遺伝子パネル検査は1回56万円(自己負担3割で16万8000円)で、がんと診断された人がすべてこの検査を受けると莫大な医療費がかかること、人手が足りないことなどから、政府は保険適用の対象を拡大することをためらっているわけですが、「がんと診断されたらパネル検査」とする方が治療効果が上がり、がんの進行や再発も抑制でき、治療費や入院費も減って、患者さんの利益が大きいだけでなく、国民総医療費も下げられるのではないかと考えます。
さらに指摘しておきたいのが、コンパニオン診断薬やがん遺伝子パネル検査は調べる遺伝子の種類が決まっていて、その中に含まれていない遺伝子異常は見つけられない、という点です。
実際、がん遺伝子パネル検査で調べても原因がわからず、がんが進行する患者さんが東京大学医科学研究所病院に来院され、全ゲノム解析でエピジェネティックな(DNA配列に依存しない)遺伝子異常を発見することができ、合う薬が見つかって全快された例がありました。また、急性白血病の若い男性患者さんが全ゲノム解析の後の論文検索によって世界でもまれなタイプの遺伝子異常を持っていること、また、抗がん剤での治療後にはその遺伝子異常が消失していたことから、骨髄移植は不要で経過観察のみでよいとわかった例もあります。
全ゲノム解析のコストは遺伝子シーケンサーやコンピューターの発展で年々下がり、機器の小型化やクラウドでのデータ保存などで大きなインフラも不要になっています。解析する遺伝子数の増加で負担が増えるエキスパートパネルの仕事は、近い将来、AIによる支援で効率や精度を上げることができるでしょう。
先進医療に全ゲノム解析のための新しい枠組みを作り、検査費用は患者さん負担にして、がん遺伝子パネル検査の扱いに慣れているがんゲノム中核拠点病院などから全ゲノム解析を採り入れていくことで、今の患者さんにも未来の患者さんにも恩恵があると考えます。
すでに世界には、ゲノム医療を政策として採り入れ、がんと診断されたら全ゲノム解析が受けられるように制度が整っているいる国もあります。
日本では、来年度に「全ゲノム解析等実行計画2022」1に基づき、がんや難病などの患者さんの全ゲノム解析を統括する組織が立ち上がる予定です。さらには、全ゲノム解析だけでなく、その結果を生かせるよう新薬の承認や既存薬の適用拡大をしやすくする仕組みづくりも進められつつあります。ゲノム医療の研究のみならず、新しい治療法を開発し、患者さんへの治療での還元を目的とする制度設計になることを願っています。私自身もその制度に資するシステムづくりや人材育成に注力します。
1 厚生労働省「全ゲノム解析等実行計画2022」
(https://www.amed.go.jp/content/000128700.pdf)
東京医科歯科大学 特任教授
東京医科歯科大学 M&Dデータ科学センター長
宮野 悟
1977年九州大学理学部数学科卒業。理学博士。1993年九大理学部教授、1996年東京大学医科学研究所ヒトゲノム解析センター教授、2014年ヒトゲノム解析センター長、2015年神奈川県立がんセンター総長などを歴任。2020年から東京医科歯科大学に新設されたM&Dデータ科学センター長。国際計算生物学会(ISCB)ISCB Fellow。2016年度上原賞(「先端ゲノミクスによる癌の分子基盤の解明」)、2019年度ヘルシーソサエティ賞(パイオニア部門)受賞、2023年度大川賞(「スーパーコンピュータを活用した全ゲノム解析、がんゲノム研究の先進的な研究」)受賞。